


A recent study by Rockpointe demonstrated the value of CME to atrial fibrillation (AFib) patients and the physicians who treat them, while also confirming the need for additional hands-on education to the broader audience of clinicians. The study, Impact of Continuing Medical Education on the Recognition of Silent Atrial Fibrillation and Mitigation of Atrial Fibrillation-related Stroke Risk, worked with primary care physicians (PCPs) and other healthcare professionals who treat patients who have stroke-associated risk factors and might also have AFib.
Rockpointe analyzed outcomes from three live activities in conjunction with chapter meetings of the American College of Physicians, three live activities at Medical Education Exchange (MEDX) Regional Conferences, and an online enduring webcourse hosted on Primary Issues. The live activities drew more than 1,300 participants, and nearly 1,200 learners viewed the webcourse. The education’s impact was assessed by comparing pre- and post-activity test scores, which indicated that participants were roughly 50% more likely to deliver evidence-based care for AFib after the activity, potentially improving care during more than 12,000 AFib patient-visits each month.
Before the education, 58% of participants were unfamiliar with at least half of the material presented. Based on clinician responses to knowledge questions, the overall pre-test score was 63%, while the overall post-test score was 94%; P<0.05.
Participant evaluations also suggested the education was highly effective. Of the 1,125 participants who responded to the evaluation, 99% agreed that the activity provided strategies to improve their practices and better prepared them to care for their patients.

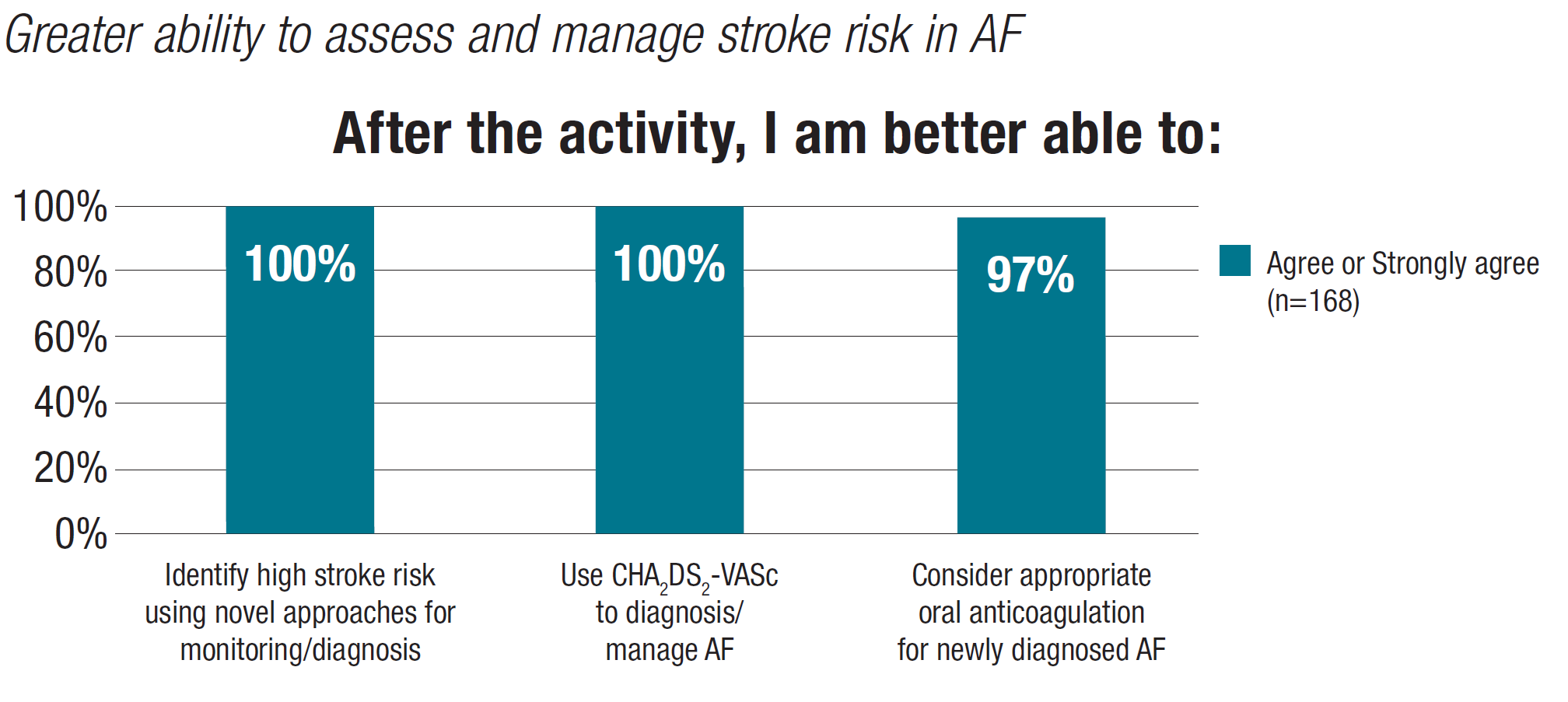
Participants became more confident in their ability to identify patients at high risk of stroke using novel approaches and in using CHA2DS2-VASc to diagnose/manage AFib and select oral anticoagulant therapy for newly diagnosed AFib. They also expressed an intention to incorporate this information into their practices.

Pre-test scores also confirmed the need for more education to the broader target audience on the following subjects:
- Identifying patients at high risk for stroke who have not been diagnosed with AFib;
- Using the CHA2DS2-VASc Risk Score; and
- Individualizing oral anticoagulant (OAC) therapy in patients with AFib.
One approach for early identification of AFib is to conduct routine electrocardiogram (ECG) screening, but such screening is not a good tool to detect sporadic infrequent events that are often silent or asymptomatic. Studies using various ECG monitoring apps have established that prolonged ECG monitoring increases the yield of AFib detection. A further complication is the fact that stroke risk scores are seldom calculated in real-world settings; therefore, clinicians are often unfamiliar with their use or have insufficient time to determine a patient’s risk score.
To help close this gap in care and further address the educational needs identified by the outcomes analysis, Rockpointe has proposed a new CME/MOC-eligible initiative, “In-home Screening for Atrial Fibrillation: CME Workshop and Real-world Application in Patient Care,” which will include a live workshop to demonstrate the effectiveness of prolonged use of a noninvasive ECG-monitoring device and associated app. Patients have expressed a preference for hand-held ECG screening devices, and there are now several FDA-approved patient devices/apps that are noninvasive, mobile, and patient-controlled.
In this workshop, participating clinicians will be shown how to use personal ECG-monitoring devices, associated apps, and accessories. They will learn how to read and interpret the ECG records obtained from their patients who are using these devices and apps in the community. They will also be encouraged to apply CHA2DS2VASc to patients with diagnosed AFib to determine whether oral anticoagulation is required.
After the workshop, a group of 100 volunteer physicians will each receive five mobile ECG screening devices to take back to their practices. These clinicians will provide the devices to a select number (~5) of their patients with a CHA2DS2VASc score of ≥2. In this exercise, a total of ~500 patients will be instructed to self-monitor their ECGs with 30-second recordings made twice daily for a two-week period. The data that the patients record will be centrally processed, and results will be transmitted back to the volunteer physicians for reading and analysis. The data will be analyzed to determine how many new AFib events the devices detected, what the CHA2DS2VASc risk score was for each identified patient, and what treatments were prescribed.
The proposed education, approved by the New England Institutional Review Board, will qualify for Maintenance of Certification (MOC) part 4, for education that has a direct impact on clinical practice. Specifically, this type of practical, hands-on, patient-focused education will lead to quantifiable changes in identifying high-risk patient populations and evaluating the prospects for prolonged ECG monitoring. The ultimate goal is to identify asymptomatic AFib in high-risk patients and to implement clinical-practice decisions to reduce the risk of ischemic stroke.
AFib is the most common heart rhythm disorder and increases the risk of stroke; however, approximately one-third of people with AFib are asymptomatic and remain undiagnosed. Therefore, early diagnosis of AFib must be a priority to prevent cardiovascular disease and stroke. To identify individuals with silent AFib, guidelines recommend screening patients aged ≥65 years using pulse palpation, ECG, or hand-held devices. Unfortunately, many PCPs are unaware of silent-AFib prevalence, and few test for it.
Once an individual is diagnosed with AFib, guidelines recommend quantitating stroke risk using the CHA2DS2VASc score, but PCPs often rely on clinical judgment alone. Patients not assessed using the CHA2DS2VASc score are at risk of receiving guideline-discordant care, as evidence-based management depends on scoring results. Many patients who should receive an anticoagulant are untreated, are not given the optimal evidence-based choice of oral anticoagulant (OAC), or do not receive the appropriate dose.
Rockpointe developed the above educational interventions based on these knowledge and competence gaps in order to help PCPs recognize the need to screen for asymptomatic AFib, use the CHA2DS2VASc score to assess stroke risk, and improve their knowledge about OACs to individualize the management of their patients with AFib.
Through effective continuing medical education, Rockpointe strives to improve and advance the quality of patient care. Its educational programs have been at the forefront of new issues in healthcare, including implementing MACRA, combating the nation’s opioid crisis, and utilizing technical advances that improve care. As part of its commitment to quality, Rockpointe works to inform the continuing-education community of significant quality-improvement issues through news and analysis on Policy and Medicine. In addition, its popular Medical Education Exchange (MEDX) CME regional meetings include sessions on the basics of quality improvement and alternative payment models, as well as relevant and scientifically accurate sessions on numerous disease states. All sessions include links back to associated National Quality Priorities to reinforce the bigger picture and the triple aim of: 1) improving health and 2) lowering cost to 3) better the patient experience. At Rockpointe, education equals quality.